
Renal – Kidney Cancer
- Home
- Renal – Kidney Cancer
- Introduction
The kidneys filter the blood and the waste products are transferred through the ureters to be stored in the bladder as urine. Urine is then discharged through the urethra to empty the bladder. Kidneys play a vital role in production of blood cells from bone marrow, maintenance of blood pressure and also in Vit-D metabolism.
There are several types of cancer that can affect the kidneys. Renal cell carcinoma (RCC), is the most common form and accounts for approximately 85% of all kidney cancers. In RCC, malignant cells develop in the lining of the kidney’s tubules and typically grow into a mass called a tumour. The earlier kidney tumours are discovered, the better a patient’s chances for survival. Tumours discovered at an early stage often respond well to treatment. Survival rates in such cases are high. Tumours that have grown large or spread to other parts of the body are much more difficult to treat and present a greatly increased risk to patients life.
- Symptoms
The symptoms of renal cancer include:
- Abdominal pain
- Haematuria: presence of blood in urine
- Palpable abdominal mass
- New onset Irreducible varicocele in a man
- Dilated blood vessels on the abdominal wall.
- Investigations
In order to accurately determine whether or not a patient has cancer, a physical examination and a number of other tests are required so that the Doctor can rule out any other conditions.
More than half of all patients with RCC have haematuria or blood in their urine. Often this blood is present in such small amounts or so diffused in the urine that it cannot be seen with the naked eye (non-visible haematuria).
- Blood tests
Complete blood picture, Renal function and in some circumstances blood tests to assess the extent of cancer( Serum Calcium, LDH levels, Liver function tests)
- Intravenous Pyelogram (IVP)
A special dye is injected your arm that travels through the bloodstream to the urinary tract, which in turn is then picked up through an x-ray. This process allows a doctor to see if there are any abnormalities in the kidney or any other damage to the organ.
- CT Scan
CT scans are special x-rays that show the internal organs of your body. Dyes are also injected allowing the doctor to see the area more clearly.
- Cystoscopy / Ureteroscopy
Blood in the urine can be caused by problems in the kidneys, ureters, bladder or the prostate. To differentiate these and identify, the doctor may order a cystoscopy or ureteroscopyto determine precisely where the internal bleeding is occurring. In cystoscopy/ ureteroscopy, a long, thin, rigid or flexible optical scope is inserted through the urethra and into the bladder. The doctor then makes a visual examination of the urethra, bladder, and kidneys to locate the site of bleeding.
- Fine Needle Biopsy
If a tumour has been diagnosed, the doctor may take a biopsy of cells to be examined in the laboratory.
- Staging and pathology:
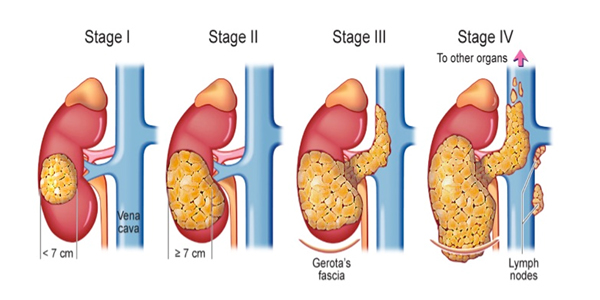
There are four main categories that make up RCC tumours based on their appearance under microscopic examination:
- Clear cell
- Granular cell
- Mixed clear and granular
- Sarcomatoid or spindle type
- Treatment Options
There are a number of treatment options for Kidney cancer; the ideal treatment depends on a number of factors, including the extent of the tumour and the current health of the patient. Treatment options vary and these should be discussed with the doctor to identify which is the best course of treatment for individual patients. They include Surgery, Chemotherapy and in very rare situations include Radiation Therapy.
- Radical Nephrectomy
The most common form of surgery for RCC, radical nephrectomy involves removal of the entire kidney, often along with the attached adrenal gland, surrounding fatty tissues and nearby lymph nodes (regional Lymphadenectomy), depending upon how far the cancer has spread.
- Partial Nephrectomy
It may be possible to remove only the cancerous tissue and part of the kidney if the tumor. A partial nephrectomy may be the procedure of choice for patients with RCC in both kidneys and for those who have only one functioning kidney.
- Laparoscopic Nephrectomy
Laparoscopic techniques allow the kidney to be removed using three 1cm “key hole” incisions in the abdomen. Occasionally 1 or 2 additional retraction ports (usually 5mm only) may be required.
- Advantages of Laparoscopic Nephrectomy
The main advantage of laparoscopy is the reduction of pain and post-operative recovery time. The patients usually can mobilise unassisted two days post-op and often are ready for discharge at that time. Patients receiving the open operation usually cannot walk until day 4 or 5 and are not ready for discharge until a week or 10 days after surgery.
Most patients after laparoscopic nephrectomy are able to return to normal activities by the end of the first week, while patients after the open operation usually take 6 to 8 weeks.Overall, reported complications from laparoscopic nephrectomy are comparable to that of open surgery and the advantages far outweigh the disadvantages.
- Robotic partial nephrectomy /Radical nephrectomy
Robotic surgery is the new modality of treatment for renal cancer, which combines the advantages of open and Laparoscopic surgery. Because of the robot and its manoeuvrability and 3-D vision the surgeon is able to perform complex minimally invasive laparoscopic surgeries with ease.